Breaking the Chain of Infectious Disease Transmission in a Retail Foodservice Business

One of the most difficult challenges in the safe operation of a retail foodservice establishment is preventing employees from working while sick. The greatest risk (from both the hazard and probability) is due to employees working while sick with the infectious disease norovirus. In fact, the most common cause of foodborne illnesses in foodservice establishments in the United States, norovirus, occurs due to significant challenges to detect and then exclude all employees who are sick because:
• A manager often cannot tell when an employee is sick via signs of illness if they do not tell them they are sick (signs of illness can be observed by others while symptoms must be measured or reported) unless they physically vomit in the restaurant or you observe they are going to the restroom two to three times an hour (a definite sign of possible illness).
• Employees can be sick but asymptomatic (up to 2 weeks after being sick as well).
• Employees may work while sick because they are not trained or provided any incentive to report illness, and/or because they need the money and cannot afford to take unpaid leave.
• Employees who are excluded from one restaurant will work at another restaurant (i.e., are employed by multiple businesses).
• Employees (when discovered sick and excluded) may have already infected other employees as they worked while asymptomatic, and if a wellness check is not performed at each shift every day, these newly infected employees will continue to work and infect others.
Now, during this coronavirus pandemic (COVID-19), the challenge of preventing virus transmission by screening and exclusion of sick employees is even greater. The impact of this new normal goes beyond whether restaurants can remain open, but even as they do, will the customers and employees feel safe from infectious diseases like COVID-19 or norovirus? It is probably now a business continuity need in the foodservice industry to perform employee screening and virus mitigation rather than an optional Standard Operating Procedure (SOP).
Viral infectious diseases like norovirus or COVID-19 are difficult to control—the viruses come into a restaurant via employees, are persistent, and are highly contagious to other employees and customers directly via surface or aerosol transmission, even in very small amounts. The two most effective controls for the prevention of both of these viral diseases in foodservice are similar:
1. The means to more efficiently reduce the risk of employees working when sick (employee screening/wellness checks)
2. The means to ensure virus mitigation using personal hygiene and environmental contamination controls (including engineering controls) to reduce the risk of virus transmission to both employees and food
The best means to ensure these processes are performed and the related hazards are controlled is by properly establishing a Process Hazard Analysis and Critical Control Points (HACCP)-based food safety management system (FSMS), whereby all the hazards are identified and controls established, employees are trained on the SOPs and managers are trained to manage them, the controls are monitored daily, and when a control is not working or absent, it is corrected in real time to significantly reduce both foodborne illness and COVID-19 transmission.[1] Development of a Process HACCP-based FSMS in a retail foodservice business based on U.S. Food and Drug Administration (FDA)’s Food Code Annex 4 on Active Managerial Control[2] is described in more detail in a new book.[3] This FSMS can also be used to include the new controls necessary to prevent COVID-19 with just a few modifications while also keeping the restaurant safe from foodborne disease outbreaks.
Viruses are often first transmitted in foodservice facilities via transmission from employees’ hands to environmental surfaces like door handles or handwash sink faucet handles.[4] The viruses are then transmitted to other employees unknowingly when they touch these common high-touch surfaces, which then leads to cross-contamination of food, often even when the employee is wearing foodservice gloves.[5] Therefore, the foodservice business’s FSMS must include the SOPs to train and screen employees for illness in an attempt to prevent this first transmission event. The FSMS must also include the SOPs for virus mitigation, which include personal hygiene controls and environmental contamination controls.
Always check with your local health department to coordinate health-related requirements to operate a foodservice business and to ensure timely and accurate information on operations. This is especially important during a sustained transmission of COVID-19 in your local area.
Employee Screening/Wellness Checks
For many years, FDA has recommended that employees be trained and screened about/for signs and symptoms of foodborne illnesses to enable their exclusion from preparing foods based on the Food Code.[6,7] However, most restaurant businesses that operate across the United States do not actually follow these recommendations until they experience/cause a norovirus outbreak. The evidence for this is clear, as these viral foodborne diseases continue to cause the most illnesses and outbreaks due to working sick employees.[8] The difficulty in correctly screening an employee for an illness, correctly deciding exclusion, and then managing that employee’s return to work can be a challenge and now even more so due to COVID-19 screening needs. Nevertheless, this works when performed properly. When combined with other controls (see below), the U.S. Centers for Disease Control and Prevention (CDC) has recommended a decision tree for protecting the public health in restaurants as they start to reopen dining areas.[9]
Foodborne-Illness Screening
The first transmission event (and the most effective control of it) starts with identifying the employee who may be sick via the signs and symptoms of a foodborne illness. For the wellness check to be effective, the foodservice business should train employees about when to report that they have these signs and symptoms and/or have received a diagnosis of any of these symptoms before they come to work. It is best to establish this training via a health policy that the employees can agree to before they begin work; it’s equally important to perform a wellness check at the beginning of every shift (perhaps when an employee clocks in). An example SOP can include:
a. Ask each employee at the time of the assessment if they have any of these symptoms:
i. Diarrhea; may also be a symptom of COVID-19
ii. Vomiting in the past 24 hours; may also be a symptom of COVID-19
iii. Fever and/or sore throat; note that fever or an employee feeling feverish is also a possible symptom of COVID-19
iv. Jaundice (yellowing of the skin or eyes)
v. Open wounds on hands/arms from cuts or burns with fever
b. Ask employees if they have been to the doctor and have received a diagnosis of any of these illnesses or pathogens:
i. Norovirus
ii. Hepatitis A
iii. Shigella spp.
iv. Shiga toxin-producing Escherichia coli
v. Typhoid fever (caused by Salmonella Typhi)
vi. Salmonella (nontyphoidal)
c. If any employee has these symptoms or has received a diagnosis of these infectious diseases or pathogens, they should be excluded from work and placed on the sick log; the only exception to this recommendation is when an employee has open wounds on hands or arms, these wounds are not releasing any body fluids, and it is feasible for the wounds to be covered with medical bandaging; in such cases, it is best that the employee be restricted from preparing and serving foods until the wounds are healed.
d. Check to ensure no employee who has been excluded from work is actually working during the shift by consulting the sick log to ensure that the sick employee does not return to work before allowed.
It is important to use a sick log (Figure 1) to track all employee exclusions, including the employee’s name and the date they are excluded from work, due to the signs and symptoms of foodborne illnesses and COVID-19. It is also then important to establish the policy to determine when an excluded employee may return to work.[10] A sick log can also help ensure an excluded employee is not placed on the work schedule until they have met the criteria to return to work and are removed from the log. This is even more important now due to COVID-19 and the resultant federal and state rules, many of which may be enforced by state and local health departments.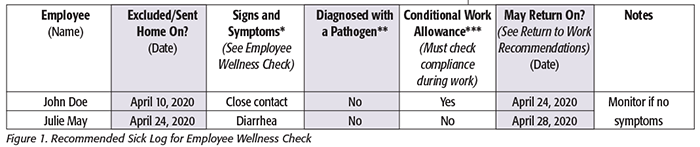
Returning to Work after Foodborne Illness
Allowing employees to return to work after exclusion with a possible or diagnosed foodborne illness depends on several factors. Each of the most common foodborne pathogens has unique characteristics of illness in humans. How long pathogens are shed in the stool and vomit affects when a food employee can return to work. Considerations for the manager include: Was the employee asymptomatic? Is medical documentation required? And is a regulatory authority approval required before they are allowed to return to work? The following recommendations are based on best practices and aligned to the most current Food Code.[7]
Signs and Symptoms
Vomiting: may return to work after 24 hours with no symptoms and was not diagnosed with a foodborne illness.
Diarrhea: may return to work after 72 hours with no symptoms and was not diagnosed with a foodborne illness. Any employee with chronic diarrhea must have medical documentation that the employee is not infectious before returning to work, as diarrhea may also be a symptom of COVID-19.
Jaundice: may return to work only after receiving medical documentation and regulatory authority approval that the employee is no longer infectious.
Fever and/or sore throat: may return to work if no other symptoms and no fever without the use of fever-reducing medications for 24 hours. Note that fever or an employee’s feeling feverish is also a possible symptom of COVID-19, so ensure that you carefully consider COVID-19 return-to-work criteria as well.
Diagnoses
Norovirus: may return to work only after no symptoms for 72 hours and upon receiving medical documentation and regulatory authority approval that the employee is no longer infectious.
Shigella: may return to work only after no symptoms for 7 days or upon receiving medical documentation and regulatory authority approval that the employee is no longer infectious.
Salmonella Typhi: may return to work only after no symptoms for 14 days or upon receiving medical documentation and regulatory authority approval that the employee is no longer infectious.
E. coli O157:H7: may return to work only after no symptoms for 7 days or upon receiving medical documentation and regulatory authority approval that the employee is no longer infectious.
Hepatitis A: may return to work only after receiving medical documentation and regulatory authority approval that the employee is no longer infectious.
Note: See the most current Food Code for recommendations on additional history of exposure and past-illness return to work, and use FDA’s Retail Food Protection: Employee and Personal Hygiene Handbook[11] as a reference to develop your employee health policy. You should also monitor these FDA resources for updates on foodborne illnesses transmitted through food, including FDA-recommended exclusion and restriction-from-work recommendations.
COVID-19 Illness Screening
If an employee or health practitioner/health department contacts the business that this or another employee has been diagnosed with COVID-19, you should exclude this employee from work, place their name on a sick log, immediately perform disinfection [using a U.S. Environmental Protection Agency (EPA)-approved disinfectant] of all high-touch environmental surfaces, have all employees wash hands, and not allow the sick employee to return to work until they meet all COVID-19 return-to-work requirments.
If an employee is confirmed to have COVID-19 via testing, you should inform fellow employees of their possible exposure to this virus in the workplace but maintain confidentiality and follow local health department guidelines related to closure of the facility. If you remain open, continue to perform wellness checks of signs and symptoms of all employees at each shift, continue to disinfect high-touch surfaces, and have employees wash hands every hour. The most current symptoms can be found on CDC’s COVID-19 website. An SOP can include:
a. Feeling sick?
i. Ask employee if they are feeling sick with acute respiratory illness that may include one or more of these symptoms: body aches (on and off), muscle pain, fatigue, headache, chills, occasional coughing, nasal congestion, runny nose.
ii. Ask employee if they are treating any of these symptoms with medicines (paracetamol/acetaminophen/ibuprofen/aspirin/cough suppressants/decongestants).
b. Fever and/or sore throat?
i. Ask employee if they are feeling feverish or have had a fever of 100.4 oF or greater in the last 24 hours checked with an oral thermometer and/or if they have a sore throat.
c. Cough/shortness of breath?
i. Ask employee if they have a cough, are sneezing more than normal, and/or have shortness of breath.
d. Diarrhea?
i. Ask employee if they have or had diarrhea in the last 48 hours.
e. Nausea or vomiting?
f. New loss of taste or smell?
g. Close contact with a sick person? A potential close-contact exposure means being a household contact of or having close contact within 6 feet for a long period (e.g., > 30 minutes without a mask) with an individual with confirmed or suspected
COVID-19. The time frame for having close contact with an individual is 48 hours before the individual became symptomatic. Critical infrastructure employees who have had an exposure but remain asymptomatic may continue to work as long as they follow conditions provided by CDC (www.cdc.gov/coronavirus/2019-ncov/community/critical-workers/implementing-safety-practices.html) prior to and during their work shift. However, it is recommended that you also confirm that:
• The employee is essential to the business (can you not manage without this employee?)
• The employee did not have high level of exposure (not living with someone that has tested positive for COVID-19
• You can effectively control this risk in the workplace (following these conditions)
If the employee has been diagnosed with COVID-19 or any of these symptoms, exclude the employee from work and place the employee on a written sick log that other managers may check to ensure the excluded employee does not return to work. The CDC guidance for when employees may return to work after being diagnosed with COVID-19 can be found here: www.cdc.gov/coronavirus/2019-ncov/hcp/disposition-in-home-patients.html. Provide the employee with this information recommended by the CDC: www.cdc.gov/coronavirus/2019-ncov/downloads/sick-with-2019-nCoV-fact-sheet.pdf.
The conditions under which critical infrastructure employees exposed to persons with suspected or confirmed COVID-19 are allowed to work include the following:
1. Prescreen: Employers should measure the employee’s temperature and assess symptoms prior to their starting work. Ideally, temperature checks should happen before the individual enters the facility (see “Conducting Employee Temperature Checks”).
2. Regular Monitoring: As long as the employee doesn’t have a temperature or symptoms, they should self-monitor under the supervision of their employer’s occupational health program.
3. Wear a Mask: The employee should wear a face mask at all times while in the workplace for 14 days after last exposure. Employers can issue face masks or can approve employees’ personal cloth face coverings in the event of shortages (Figure 2).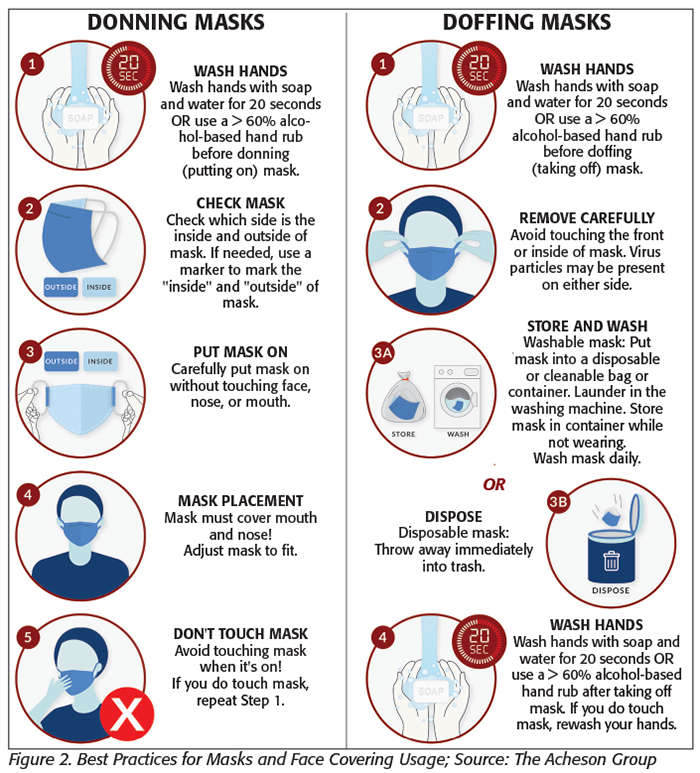
4. Social/Physical Distancing: The employee should maintain 6 feet and practice physical distancing as work duties permit in the workplace.
5. Disinfect and Clean Work Spaces: Clean and disinfect all areas such as offices, bathrooms, common areas, and shared electronic equipment routinely.
Immediately perform disinfection (using an EPA-approved disinfectant) of all high-touch environmental surfaces and thereafter every hour, and have all employees wash hands and thereafter every hour.
COVID-19 Return to Work
The decision to allow an employee to return to work after exclusion based on signs and symptoms of COVID-19 alone should be made in the context of the local regulatory authority requirements using time-since-illness onset and time-since-recovery date. Considerations for the person in charge include: Did an employee suspected as having COVID-19 based only on signs and symptoms self-isolate for 14 days? Did the employee receive a diagnosis of COVID-19 via testing (some areas may not be able to test for confirmation; testing also determines whether a person is probably infectious and shedding the virus)? Did an employee test positive for COVID-19 but not have any signs and symptoms (i.e., infected but no disease)? Always check the most current CDC guidance based on testing results and/or signs and symptoms only for return-to-work recommendations specific to businesses.
Signs and Symptoms (not diagnosed by a medical practitioner)
• Feeling sick or having a fever and/or sore throat, cough, chills, muscle pain, or shortness of breath: may return to work after 14 days
• AND at least 3 days after no symptoms, including fever, cough, and shortness of breath
• AND at least 10 days have passed since the first signs and symptoms first appeared
Close Contact with a Sick Person (including if the close contact tested positive)
Employees excluded who did not work under the CDC conditional work allowance may return to work after 14 days if they have neither developed nor currently have any of the COVID-19 signs and symptoms.
Diagnosed (tested positive with or without signs and symptoms)
• Employees tested positive with no signs or symptoms
° Employees who did not develop any symptoms of COVID-19 after testing positive may return to work after at least 10 days have passed since the date of their first positive coronavirus diagnostic test
° AND they do not have any signs and symptoms
• Employees tested positive with signs and symptoms
May only return to work after:
° Resolution of fever without the use of fever-reducing medications
° AND improvement in respiratory symptoms
° AND negative results of an FDA Emergency Use Authorized molecular assay for COVID-19 from at least two consecutive nasopharyngeal swab specimens collected at least 24 hours apart. All test results should be final before isolation is ended. Testing guidance is based upon limited information according to the CDC and is subject to change as more information becomes available. In persons with a persistent productive cough, SARS-CoV-2 RNA might be detected for longer periods in sputum specimens than in upper respiratory tract (nasopharyngeal swab) specimens
Note: Ensure that the person in charge/manager continues to monitor each employee’s wellness before and during each shift to determine whether any of these conditions change.
Virus Mitigation
Based on what is currently known about COVID-19, transmission from person to person happens most frequently among close contacts (within about 6 feet) via respiratory droplets, and the virus is not spread via food. Thus, ensuring personal hygiene controls are in place is critical to the prevention of COVID-19 transmission from person to person. These controls will also reduce the risk of transmission to environmental surfaces and prevent cross-contamination of food with foodborne pathogens like norovirus (e.g., when a sick employee with norovirus handles food with these controls in place).
Transmission of COVID-19 to persons from surfaces (person to surface to person) contaminated with the virus has not been well-documented but is likely to occur based on evidence from how other respiratory pathogens are spread (after an employee touches a contaminated surface and then touches their eyes, nose, or mouth). Current evidence suggests that COVID-19 may remain viable for hours to days on surfaces made from a variety of materials.[9] Thus, ensuring environmental contamination controls are in place is critical to the prevention of COVID-19 from person to surface to person. These controls will also reduce the higher risk of transmission of norovirus to foods. Cleaning of visibly dirty surfaces followed by disinfection is the most effective means to reduce transmission of viruses and other pathogens from high-touch surfaces in foodservice settings.
Personal Hygiene Controls
These controls are necessary to reduce the spread of pathogens (viruses like SARS-CoV-2 or norovirus shed by employees) from employees/customers to employees and food:
• Enable personal-space distances of 6 feet or more between working employees in the kitchen and employee/customer service areas. Use colored tape to mark off distances between work spaces, including between service areas and customer interactions.
° Provide signage to caution customers to remain 6 feet apart (no lines) during service.
° If a personal space distance of 6 feet or more is not practical at all times, then use “time in place” limits to reduce the amount of time an employee may be within this distance and ensure employees wear a cloth mask at all times.
• Provide single-use disposable cloth masks/face coverings to employees or allow use of personal cloth masks/face coverings. CDC recommends all restaurant employees wear masks/cloth face coverings, especially in areas of significant community-based transmission. CDC also advises the use of simple cloth face coverings to slow the spread of the virus and help people who may have the virus and do not know it avoid transmitting it to others. Cloth masks/face coverings fashioned from household items or made at home from common materials at low cost can be used as an additional, voluntary public health measure. Cloth masks/face coverings should not be placed on anyone who has trouble breathing or is unconscious, incapacitated, or otherwise unable to remove the mask without assistance. The cloth masks/face coverings recommended are not surgical masks or N-95 respirators. Those are critical supplies that must continue to be reserved for healthcare workers and other medical first responders, as recommended by current CDC guidance.
° The proper use of cloth masks/face coverings is demonstrated in Figure 2.
• Promote frequent and thorough handwashing (every hour), including by providing employees and customers with a place to wash their hands. If soap and running water are not immediately available, provide alcohol-based hand rubs containing at least 60 percent alcohol.
° Additional times to wash hands or use hand rubs include after an employee blows their nose, coughs into their hands, or sneezes, after using the restroom, before preparing food, and between glove use.
• Provide alcohol-based sanitizer of 60 percent or more alcohol at all customer service locations so that employees can use it between each high-touch event during service transactions where handwash sinks are not easily accessable (e.g., outside performing drive-through service).
° High-touch events include touching money, credit cards, smartphones, door handles, payment systems/touch screens, shared pens, after handling any other materials handled by customers (e.g., reusable bags), and after receiving and storing products from delivery services.
• When gloves are used, especially for continuous service of packaged foods to customers, replace gloves whenever used to touch anything other than the packaged foods.
° Gloves should be replaced often, especially when likely in contact with materials handled by customers.
° A best practice for reducing pathogens such as coronavirus on gloves (ONLY during service of packaged foods for delivery/pickup/drive-through) is to periodically sanitize the gloves with a surface sanitizer or alcohol-based hand rub. Be sure the gloves are compatible with the sanitizer before use.
° Establish a glove-use management system5 to ensure gloves are not a contributing factor to the spread of infectious diseases like COVID-19 or norovirus.
• Provide additional barriers if feasible between employees and customers.
° Install physical barriers, such as clear plastic sneeze guards, and/or install a window for customer service only with opening for transfer of product/payment.
• Employees should avoid touching their eyes, nose, and mouth.
• Encourage employee respiratory etiquette, including covering coughs and sneezes with their arms or paper towel/wipe.
• Discourage employees from using other employees’ phones, pens, closed offices, or other tools and equipment unless cleaned and disinfected between uses.
• Employees should avoid close contact with people who are sick when not at work and call their manager/supervisor if contact occurs before coming to work.
Environmental Contamination Controls
These controls are necessary to kill and/or remove pathogens (viruses like coronavirus or norovirus shed by employees) on high-touch surfaces and in the air[12] to prevent the spread from employees/customers to other employees/customers or food. It is important to train employees on the differences between cleaning and sanitation and cleaning and disinfection, and not allow employees to use disinfectants on food contact surfaces unless the disinfectant is EPA-registered as a no-rinse food contact chemical. “Cleaning” refers to the removal of dirt and impurities, including some pathogens, from surfaces. Cleaning alone does not kill most pathogens. But by removing pathogens, it decreases their number and therefore some risk of spreading them. Disinfecting works by using chemicals to kill pathogens on surfaces. This process does not necessarily clean dirty surfaces. But killing pathogens remaining on a surface after cleaning further reduces any risk of spreading them.
Maintain consistent cleaning and disinfection practices, including hourly cleaning and disinfection of high-touch surfaces in the work environment (unless an employee has tested positive for COVID-19). Employers must ensure employees are trained on the proper methods of cleaning and disinfection, the hazards of the cleaning and disinfection chemicals used in the workplace in accordance with the Occupational Safety and Health Administration’s Hazard Communication standard (29 C.F.R. 1910.1200), and provide employees with personal protective equipment when required (PPE, such as protective eyewear).
• Separate the cleaning and disinfection tools and SOPs, and do not use reusable cloth towels for the cleaning and disinfection of surfaces during COVID-19. CDC recommends single-use disposable wipes for disinfecting surfaces, if available. There is a risk of cross-contamination of foods when using reusable towels[13] that may also be likely to spread COVID-19 when they’re used to clean and disinfect high-touch surfaces.
• Cleaning staff should wear disposable gloves for all tasks in the cleaning process, including handling trash. Gloves should be compatible with the disinfectant products being used. Additional PPE might be required based on the cleaning/disinfectant products being used, and whether there is a risk of splash. Gloves should be removed carefully to avoid contaminating the wearer and the surrounding area. Employees must wash their hands after removing gloves.
• If high-touch surfaces are dirty, they should be cleaned using a detergent or soap and water prior to disinfection.
• For disinfection, use only disinfectants that will kill COVID-19 found on the EPA list at www.epa.gov/pesticide-registration/list-n-disinfectants-use-against-sars-cov-2. Check the EPA label of your current disinfectant if it is not on the list. Disinfectant products that kill norovirus will most likely kill COVID-19, especially if they have 70 percent alcohol or state that the product kills SARS/MERS on the label. Follow the manufacturer’s directions on use and “time to kill” or “contact time” requirements to ensure the product is left on the surface wet with enough time to kill the viruses.
• Clean and disinfect all handwash and other sink faucet handles in restrooms, kitchen, and service areas, and encourage employees to not touch doorknobs/handles if feasible but to disinfect after use.
• If your establishment is in a high-transmission area (defined by your state and/or local health authorities), you should escalate the times you clean and disinfect all high-touch surfaces.
When an employee is excluded due to COVID-19 symptoms or an employee who has worked in the last 48 hours has tested positive for confirmed COVID-19, the following should be performed:
• Close off areas used by this employee and customers and wait as long as practical (to allow air circulation to settle any viruses onto surfaces) before beginning cleaning and disinfection to minimize potential for employee and customer exposure to respiratory droplets.
° If the employee is excluded due to symptoms while at work, you may need to close the establishment temporarily to clean and disinfect high-touch surfaces.
° If an employee has worked in the last 48 hours, and you learn that this employee has tested positive for COVID-19, you may need to close the business, but you should initiate escalated cleaning and disinfection.
° In both cases, CDC recommends that you inform other employees of the exclusion without disclosing confidential information.
• Wear disposable gloves and gowns for all cleaning and disinfecting tasks, including handling trash.
• Clean and disinfect all areas visited or used by the employee, with an increased focus on frequently touched surfaces including cooking equipment buttons/handles and utensils.
• Gloves and gowns should be removed to avoid contamination after use and discarded upon removal. The employee who performs this task should wash hands after removal of the gloves and gowns.
• Any potential contamination of individuals or environment during the cleaning and disinfecting process should be reported to a supervisor.
Breaking the chain of human infectious disease transmission has always been a challenge, especially when there is no vaccine to prevent a disease like norovirus (a foodborne disease). The challenge is even greater when the infectious disease is a respiratory disease simply spread in the air. The only means to prevent both infectious diseases must be by using multiple controls (like speed bumps on a road used to slow down traffic and prevent traffic accidents) to reduce the risk of exposure and infection. The difficulty in maintaining these controls is evidenced by the spread of both diseases in the United States. Only when the most effective controls are consistently deployed, monitored, and directly managed (and an FSMS is the best means to do this) will significant reduction in infectious diseases in retail foodservice businesses occur.
These recommendations may change due to the evolving information about how COVID-19 spreads, causes disease, and what controls provide the best outcomes of prevention. All the controls to prevent foodborne infectious diseases are well-known and have been effective if they are deployed and monitored using an FSMS. Please continually check both the CDC and FDA websites for the most current guidance related to prevention of infectious diseases in retail foodservice businesses.
References
1. FDA. 2018. FDA Report on the Occurrence of Foodborne Illness Risk Factors in Fast Food and Full-service Restaurants, 2013–2014.
2. FDA. 2017. “Annex 4. Management of Food Safety Practices – Achieving Active Managerial Control of Foodborne Illness Risk Factors.” Food Code.
3. King, H., Food Safety Management Systems: Achieving Active Managerial Control of Foodborne Illness Risk Factors in a Retail Foodservice Business (Springer, 2020).
4. Duret, S., et al. 2017. “Quantitative Risk Assessment of Norovirus Transmission in Food Establishments: Evaluating the Impact of Intervention Strategies and Food Employee Behavior on the Risk Associated with Norovirus in Foods.” Risk Anal 37(11): 1–27.
5. King, H. and B. Michaels. 2019. “The Need for a Glove-Use Management System in Retail Foodservice.” Food Safety Magazine 25(3): 28–31, 56–58.
6. www.fda.gov/food/retail-food-industryregulatory-assistance-training/retail-food-protection-employee-health-and-personal-hygiene-handbook.
7. www.fda.gov/Food/GuidanceRegulation/RetailFoodProtection/FoodCode/ucm595139.htm.
8. U.S. Centers for Disease Control and Prevention. Surveillance for Foodborne Disease Outbreaks, United States, 2017, Annual Report (Atlanta: U.S. Department of Health and Human Services, 2019).
9. www.cdc.gov/coronavirus/2019-ncov/downloads/community/restaurants-and-bars-decision-tree.pdf.
10. www.emergiprotect.com/sicklog.
11. www.fda.gov/food/retail-food-industryregulatory-assistance-training/retail-food-protection-employee-health-and-personal-hygiene-handbook.
12. www.cdc.gov/coronavirus/2019-ncov/community/office-buildings.html.
13. King, H. 2018. “Is It Time to Change How We Clean and Sanitize Food Contact Surfaces with Resuable Wiping Towels?” Food Safety Magazine 24(4): 48–53.
Hal King, Ph.D., is managing partner of Active Food Safety, www.activefoodsafety.com, and a member of the editorial advisory board of Food Safety Magazine. He can be reached at halking@activefoodsafety.com.
Looking for quick answers on food safety topics?
Try Ask FSM, our new smart AI search tool.
Ask FSM →







